
What is an ACL Tear?
Dr. Jazayeri’s Personalized Approach to ACL Injuries
Each ACL tear presents uniquely in its pattern, and therefore, treatment is customized to address the specific characteristics of each individual case.
Dr. Jazayeri’s approach centers on preserving the native ACL whenever possible. Each patient is evaluated holistically—taking into account their build, anatomy, sport, position, timing in the season (or life), and the exact injury pattern. No two athletes or injuries are the same, and treatment recommendations are tailored accordingly.
Whenever feasible, a preservation-first philosophy is applied, utilizing a combination of advanced surgical techniques, biologic augmentation, and rehabilitation protocols to promote healing and expedite safe return to activity.
Treatment Options:

1. Non-Operative Management (for Partial or Low-Grade Tears)
Some partial ACL tears—especially low-grade or functionally stable injuries—may not require surgery. Select patients may benefit from a comprehensive non-operative treatment plan, which includes:
- Tailored physical therapy
- ACL specific knee bracing
- Orthobiologic therapy using Bone Marrow Aspirate Concentrate (BMAC), derived from the patient’s iliac crest, which provides mesenchymal stem cells to support biologic healing
This approach is ideal for those who maintain good functional stability and are motivated to engage in a structured rehabilitation program.

2. ACL Repair (When Feasible)
For ACL tears located near the ligament’s bony attachment (proximal), where the tissue is most amenable to healing, ACL repair is a viable option that allows preservation of the native ligament.
Key Benefits of ACL Repair:
- Maintains your natural ligament, preserving proprioceptive fibers
- No need for graft harvesting (reduces donor site pain)
- Avoids full bone tunnel drilling
- Less postoperative pain
- Faster recovery (return to sport in ~6 months)

3. ACL Reconstruction (Gold Standard)
For complete ACL tears, midsubstance ruptures, or tissue that is not repairable, ACL reconstruction remains the gold standard, especially in young, active individuals and athletes.
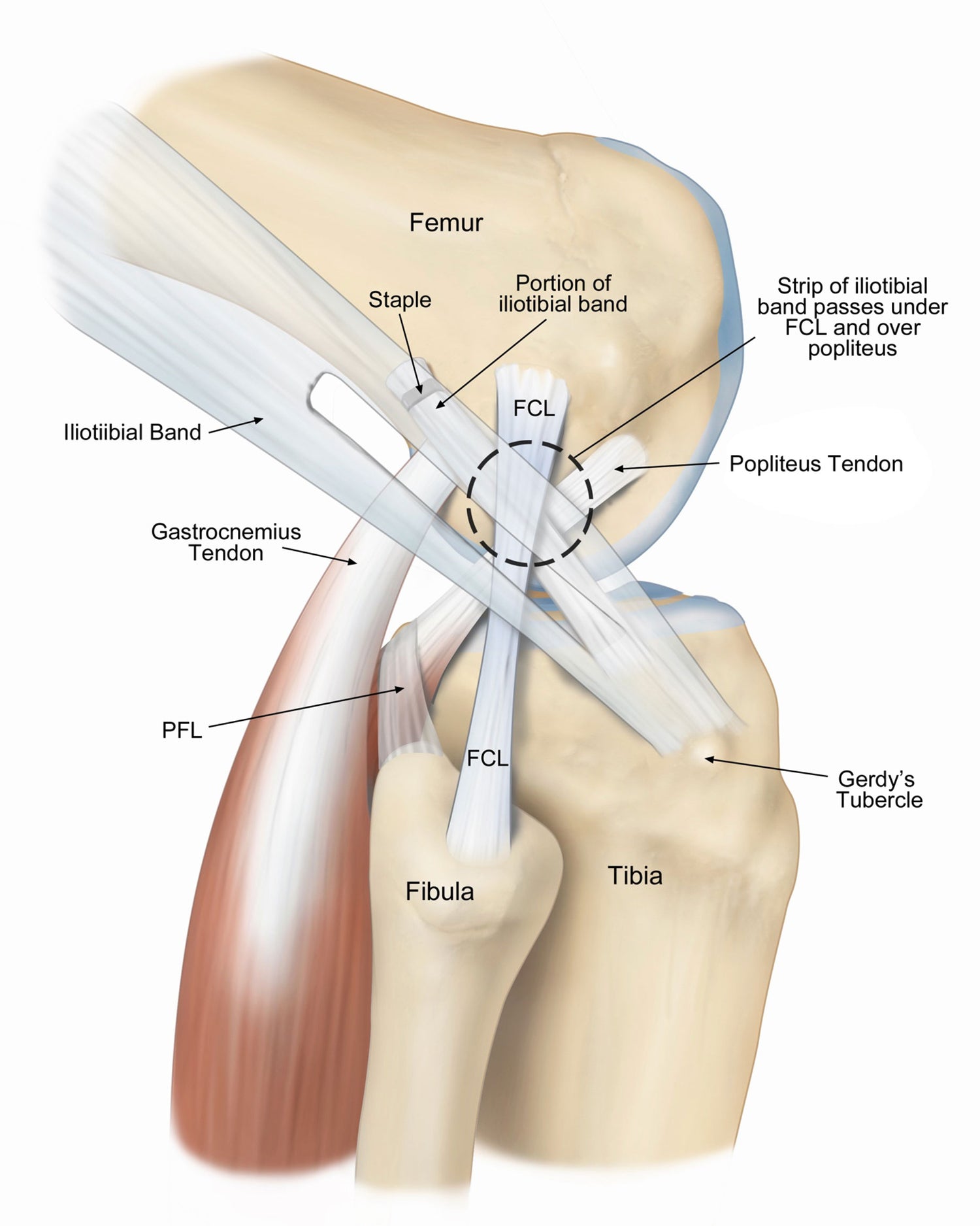
4. Lateral Extra-Articular Tenodesis (LET):
In select patients, Dr. Jazayeri may perform a (LET), a procedure that enhances rotational knee stability by using part of the iliotibial band (ITB) to reinforce the ACL.
ACL Procedure Options:
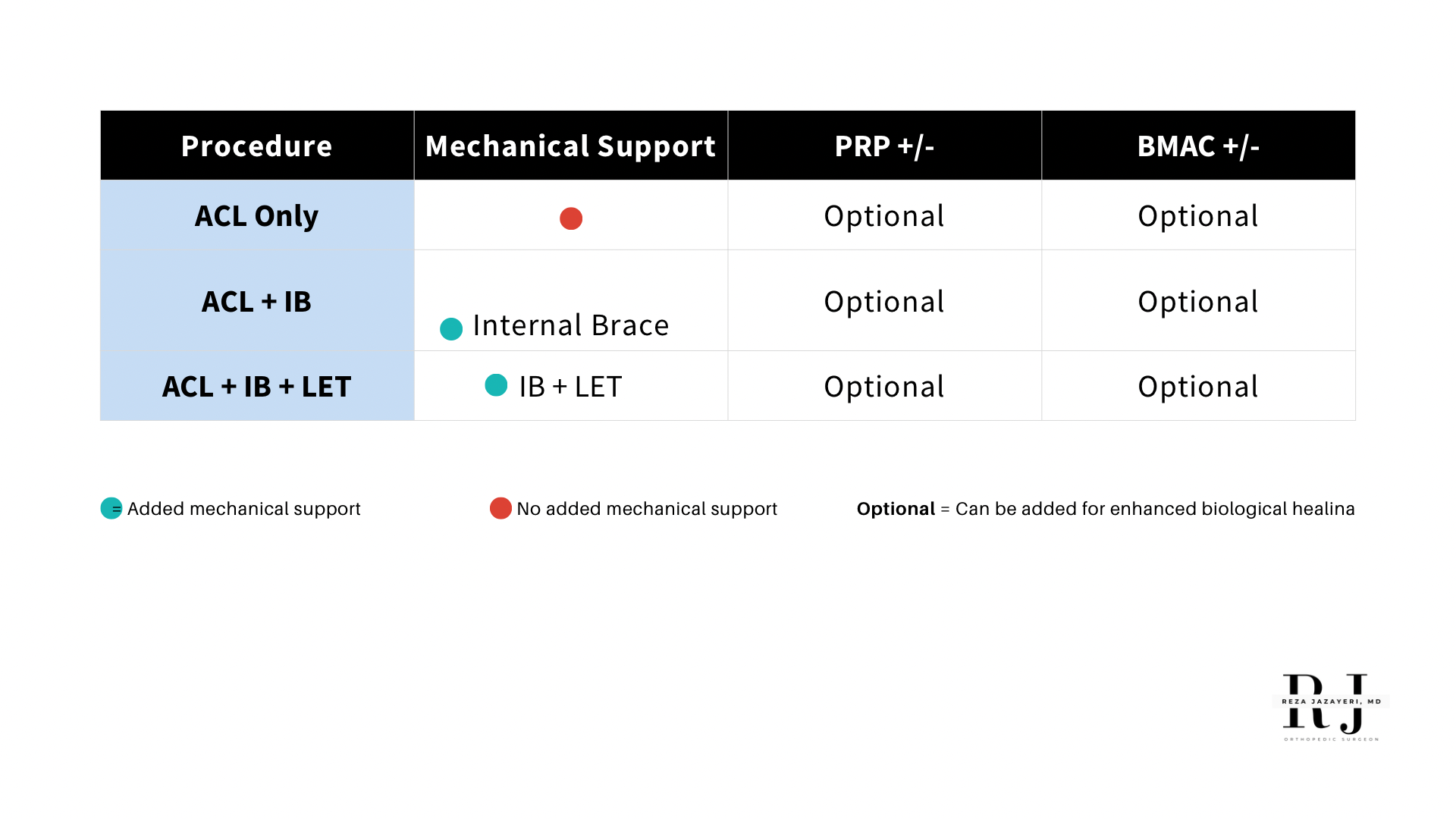

Bio-Fertilization™ Technique: Biologically Optimized ACL
A modern, comprehensive protocol to enhance outcomes and accelerate return to play.
patient resource
ACL RECONSTRUCTION POST OPERATIVE PATIENT INSTRUCTIONS CLICK HERE
What to expect with your ACL surgery.
evaluation
What Happens Next?
Whether you're a high school athlete, weekend warrior, or professional competitor, Dr. Jazayeri will guide you through your options using a personalized, evidence-based, and patient-first approach. You'll receive a plan tailored to your anatomy, sport, goals, and injury characteristics.
Key Takeaway:
- ACL reconstruction remains the most common and effective solution for complete ACL tears.
- ACL repair, when feasible, offers an exciting option for certain tear patterns—especially when biologically and mechanically augmented.
- Non-operative strategies may be appropriate for select partial tears, especially when supported by orthobiologics.
- Advanced augmentation techniques (BioBrace, BEAR, Internal Brace, BMAC) are enhancing outcomes across the board.
- Dr. Jazayeri’s BOAT protocol ensures every patient is metabolically, surgically, and rehabilitatively optimized for the best possible recovery.
Contact us
If you have questions or concerns, please don’t hesitate to ask Dr. Jazayeri or the care team: (855) 892-0919
Our goal is to relieve your pain, restore knee function, and help you return to the activities you love, safely and successfully.